|
Patients with potential rabies exposures are a relatively frequent reason for evaluation in an emergency room. Animal bites account for approximately 1% of all ER visits. Within the District of Columbia, all cats and dogs are required to be vaccinated against rabies and distemper from the age of four months, and after the initial set of shots, must be re vaccinated at least every 3 years. Not all owners may comply or have documentation readily available after an animal bite, and many patients may present after contact with a wild animal. As many residents may have already found, many tourists present after contact with squirrels, which are not known to carry rabies.  DC DOH Vaccination, Bites, & Rabies
Contact Phone: (202) 535-2323 Contact Fax: (202) 442-4817 Office Hours: Monday to Friday 8:15 am to 4:45 pm 899 North Capitol Street, NE Washington DC 20002 https://doh.dc.gov/service/vaccination-bites-and-rabies
0 Comments
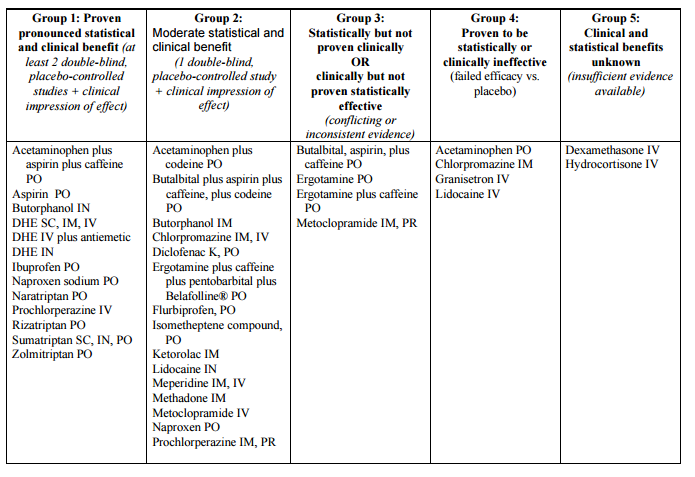 Identifying atypical headaches, treatment of primary headaches, and how to approach complicated and atypical headaches. Adapted from Sigrid Nasser's Grand Rounds lecture, January 25th, 2015
Blistering AgentsMustard Gas, Phosgene, and Lewisite are the three most prominent blister agents. These are warfare agents which are dispersed and cause severe blisters. Apart form Lewisite, there are no antidotes and treatment is supportive including decontamination. Sulfur Mustard (mustard gas) is a colorless, odorous liquid when pure, but is dispersed as a yellow/brown gas that smells like mustard when used as a warfare agent. Bullous lesions present 2-6 hours after exposure and can cause mucosal damage including the respiratory tract. Lewisite has a more rapid onset than mustard gas, and has an antidote called "British Antilewisite (BAL). Phsgene oxime has never been used in warfare, but can cause wheels with blanching welts, which turn to tissue necrosis within 24 hours.  Tear AgentsMultiple chemicals are used to cause tearing and mucosal irritation. The most commonly used are pepper-spray (capsaicin), CS (2-chlorobenzalmalononitrile), CN (mace). Pepper spray ranges from 10%-90% capsaicin depending on the product. Pepper-spray is self-limiting and shouldn't require more treatment than washing out. CN, or 'mace' and CS are both used by military and police, and typically can cause severe irritation, corneal abrasions, and even skin blistering if the patient is not decontaminated. CS is known to provide worse effects. CS can induce severe coughing and vomiting. Effects usually last for 20 minutes to an hour, and effects can persist for hours. Clothing will need to be thrown away or washed multiple times. 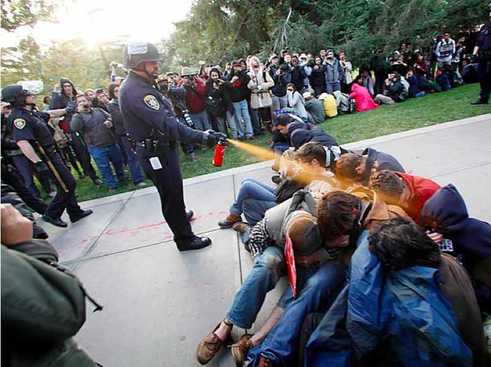 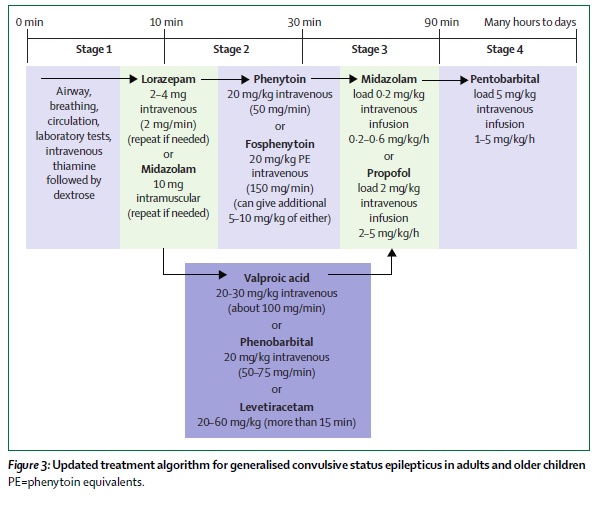 Status epilepticus is a common neurological emergency when a patient has a prolonged seizure or a series of seizures with incomplete return to baseline. The approach to status epilepticus has focused on early seizure termination, and rapid escalation of care to include general anesthesia when needed.
Status Epilepticus: A prolonged seizure or multiple seizures with incomplete return to baseline. According to an article published by the American Academy of Pediatrics in 2010, severe and fatal battery ingestions are increasing, and many patients are being treated inadequately for button battery ingestions. From 1985 to 1009, there has been a 6-fold increase in button battery ingestions with resulting major or fatal outcomes. The largest increase has been with lithium-cell batteries (24% of ingestions) and 20-25mm diameter batteries (18% of ingestions). 20mm lithium cells are the most common to be associated with severe outcomes. A high index of suspicion is needed; 54% of fatal outcomes are misdiagnosed, usually complicated by nonspecific presentations. Most serious battery ingestions are not witnessed. Consider an ingestion anytime a patient is wheezing, drooling, vomiting, or has chest pain or discomfort. 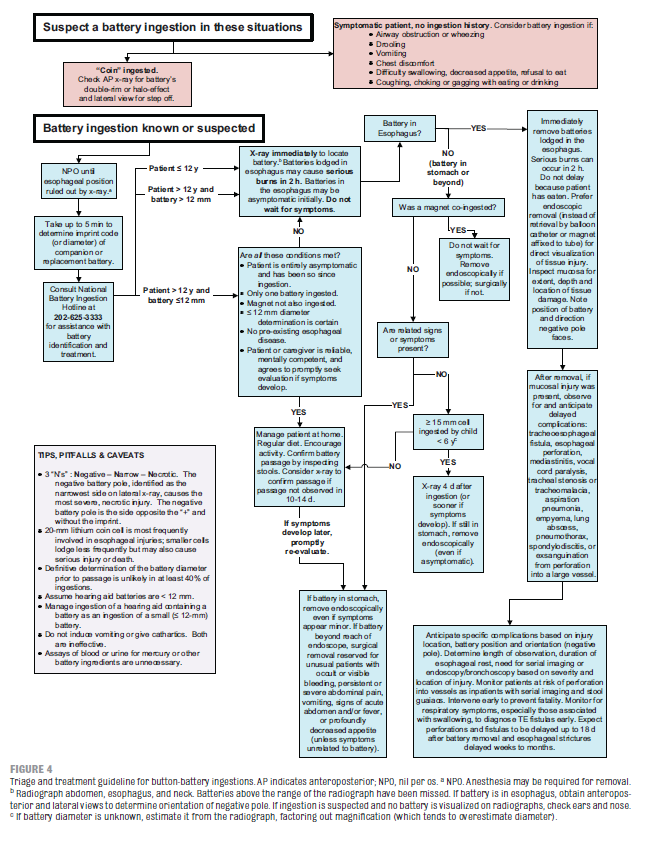 Huffing, or abusing volatile vapors to induce intoxication, is a common form of recreational drug abuse, most seriously by younger teens and homeless children. More than 1,400 household products can be used as inhalants to get high. Frequently the users inhale aerosol gases by using plastic or paper bags to concentrate the fumes. Effects of huffing range from an alcohol-like intoxication and euphoria to vivid hallucinations. Effects depend on the type and amount of substance.
Statistics on inhalant use may be significantly under-reported because deaths may be attributed to a discrete event, such as a stroke or heart attack, which may have been secondary to inhalant abuse. 10% of 8th graders have abused inhalants in the past year. There are currently an estimated 11 million people in the world infected with TB, and there were 9,412 cases in the United States in 2014. The American Thoracic Society, Center for Disease Control and Prevention, and the Infectious Diseases Society of America have all come together to create a new guideline for diagnosing pulmonary, extrapulmonary, and latent tuberculosis in adults and children.  Six common causes of ST elevation (J point 1mm above the baseline)
Evaluating for concerning causes of ST elevation:
Adapted from Andy Simmon's Grand Rounds lecture, January 11th, 2017. How to identify serious injury that requires admisison for neurosurgery or observation, and how to instruct discharged patients for recovery expectations, followup, and return precautions.  Bupivacaine and lidocaine are often used concurrently, in theory, to combine the more rapid onset of lidocaine and the longer duration of bupivacaine. However, multiple studies, including a 1996 Journal of Podiatric Medicine article and a 2013 Canadian Journal of Plastic Surgery study have found no statistical difference between the anesthetics with regard to onset of action. 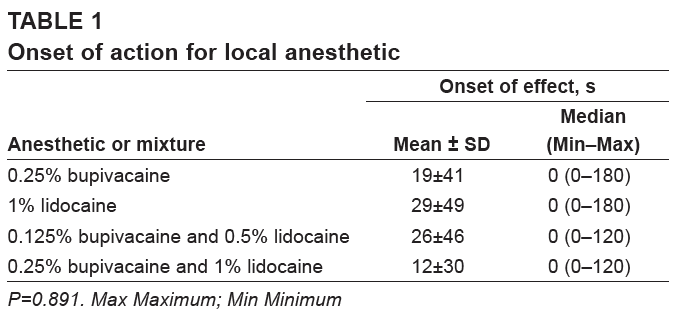
|
Categories
Archive
February 2018

Please read our Terms of Use.
|
||