 Identifying atypical headaches, treatment of primary headaches, and how to approach complicated and atypical headaches. Adapted from Sigrid Nasser's Grand Rounds lecture, January 25th, 2015 Identifying Atypical HeadachesMigraines are seen frequently in the ER, and typically present similar to the POUND Mnemonic;
Atypical headaches can be identified using the SNOOP mnemonic
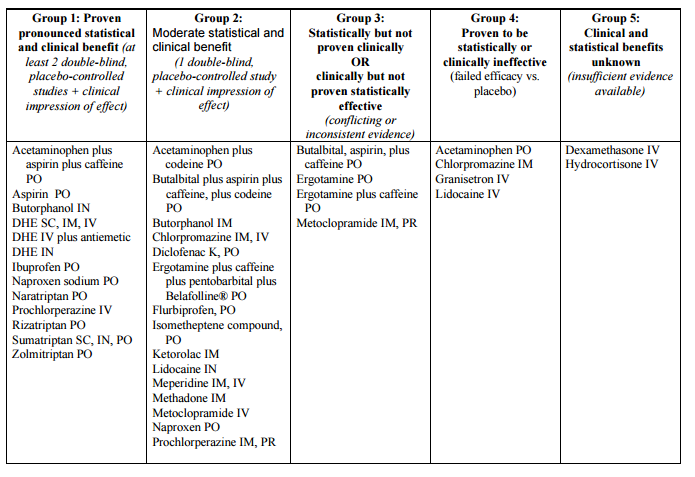
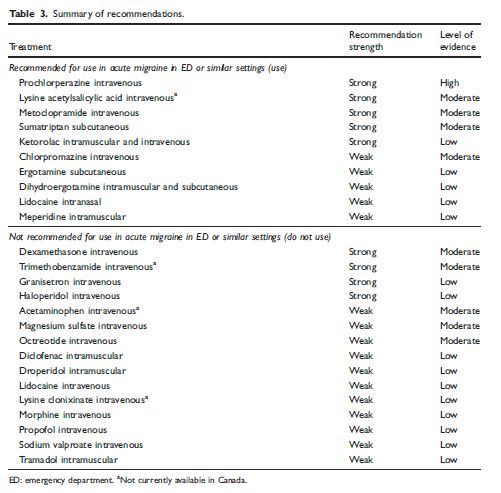
Treatment of primary headachesPatients presenting with typical headaches without red flags, and intact neurologic exams can be treated without imaging. Primarily, the goals of care are to block inflammation, hydrate, and utilization of dopamine or histamine antagonists or GABA agonists to treat headaches. Simple Analgesics: Tylenol and other NSAIDs can be used with antiepetics to treat mild-moderate primary headaches including migraines. Triptans: Although effective against placebos in studies, triptans have many limitations and contraindications, and is less frequently utilized in the emergency department. Dopamine Antagonists: Evidence shows that DA such as metoclopramide or prochlorperazine is better than toradol for primary recurrent tension headaches and migraine. Magnesium: Studies show magnesium is more effective than placebo or IVF alone. Anticholinergics: There is minimal data showing that benadryl helps with akasthisia or headaches, however patients tend to have shorter length of stay when given benadryl in addition to DAs Steroids: Dexamethasone has previously been used as an acute headache treatment and recurrence prevention. A recently American Headache society review recommends for a single dose, however, currently, a 2015 Canadian Headache Society review recommends against steroids. Fluids: There is little data to suggest that IVF are effective, however anecdotally, IVF tend to help with headaches and should be offered unless there are any contraindications.
 Secondary HeadachesCommon causes of secondary headaches include masses, bleeds, pseudotumor, hydrocephalus, hissection, carbon monoxide, and temporal arteritis. Concerns for secondary headaches includes any neurologic deficits, acute onset, new headaches in patients > 40 years old, or any signs of systemic illness or cancers.
Secondary headaches require further evaluation including imaging and potentially lumbar puncture to evaluate opening pressure and fluid evaluation. Negative CT imaging does not fully rule out masses, as well as potential central venous thrombosis. CTV can come close to the sensitivity of MRV in diagnosing venous thrombosis.
1 Comment
Karen
5/31/2024 02:20:38 am
I recommend this herbal syrup............. Leave a Reply. |
Categories
Archive
February 2018

Please read our Terms of Use.
|
||||||