SUBOXONE
(BUPRENORPHINE-NALOXONE)
General Information
| Bupe Provider Education Sheet |
WHAT ARE WITHDRAWAL SYMPTOMS/SIGNS FROM OPIOIDS?
Dilated pupils, goosebumps, sweating, runny nose, tearing eyes, diarrhea/nausea/vomiting/stomach cramps, restlessness, agitation/anxiety, tachycardia, bone or joint aches, tremor, yawning. The COWS scale (on mdcalc) helps us to grade the amount of withdrawal.
WHAT IS buprenorphine-naloxone?
Buprenorphine-naloxone is a medicine that is used to treat opioid use disorder (OUD). It’s a narcotic, so it is a substitution therapy sort of like how methadone is a substitution therapy. The main difference between them is that buprenorphine-naloxone is a “partial agonist” which means that if the dose increases, it has a “ceiling effect” and patients don’t get high. It’s also quite hard to overdose on (not impossible – usually overdosing happens because people mix it with benzodiazepines, alcohol, or fentanyl). The other main difference is that buprenorphine-naloxone is available by prescription, so people can lead a much more normal life on it, seeing a primary care doctor once a month for a prescription refill, rather than going to a methadone clinic daily.
HOW DOES IT WORK?
The goal of buprenorphine-naloxone is to prevent patients from feeling sick, while preventing the high. In the sublingual form naloxone is not active as it has low bioavailability, however if it is injected it has high bioavailability and becomes active. The naloxone is present to prevent people from dissolving the medication and injecting it as this would precipitate severe withdrawal.
WHY IS STARTING BUPRENORPHINE-NALOXONE COMPLICATED?
Buprenorphine-naloxone binds very strongly (aka “high affinity) to the same receptors as other narcotics do. Because it has such high affinity, if patients take buprenorphine-naloxone and THEN take heroin, they won’t really feel effects of the heroin because the receptors are already bound up. But if patients have other narcotics int heir system and THEN take buprenorphine-naloxone, the buprenorphine-naloxone will actually displace other narcotics from the narcotic receptor, and this will precipitate bad withdrawal symptoms and make patients feel even worse!
So, before starting buprenorphine-naloxone the patient cannot take ANY type of narcotic pain medicine for ~12 hours (or much longer if it was a longer acting narcotic, such as OxyContin, MSContin or methadone). The patient also has to be in moderate withdrawal (COWS scale score of ~8+) when starting the first dose of buprenorphine-naloxone. Since there is a lot of fentanyl in DC’s heroin supply, many of our patients with OUD will be using fentanyl without realizing it. People who use fentanyl can tend to feel withdrawal symptoms before 12 hours have passed, but you should generally still wait about 12 hours before starting the buprenorphine-naloxone to avoid precipitated withdrawal.
It is ok (and in fact, encouraged!) to give patients medications to relieve symptoms of withdrawal while waiting to start buprenorphine-naloxone. Doing so makes it more likely they can wait long enough to start safely. These may include clonidine, ondansetron, diphenhydramine, loperamide, gabapentin, NSAIDs and others.
So, before starting buprenorphine-naloxone the patient cannot take ANY type of narcotic pain medicine for ~12 hours (or much longer if it was a longer acting narcotic, such as OxyContin, MSContin or methadone). The patient also has to be in moderate withdrawal (COWS scale score of ~8+) when starting the first dose of buprenorphine-naloxone. Since there is a lot of fentanyl in DC’s heroin supply, many of our patients with OUD will be using fentanyl without realizing it. People who use fentanyl can tend to feel withdrawal symptoms before 12 hours have passed, but you should generally still wait about 12 hours before starting the buprenorphine-naloxone to avoid precipitated withdrawal.
It is ok (and in fact, encouraged!) to give patients medications to relieve symptoms of withdrawal while waiting to start buprenorphine-naloxone. Doing so makes it more likely they can wait long enough to start safely. These may include clonidine, ondansetron, diphenhydramine, loperamide, gabapentin, NSAIDs and others.
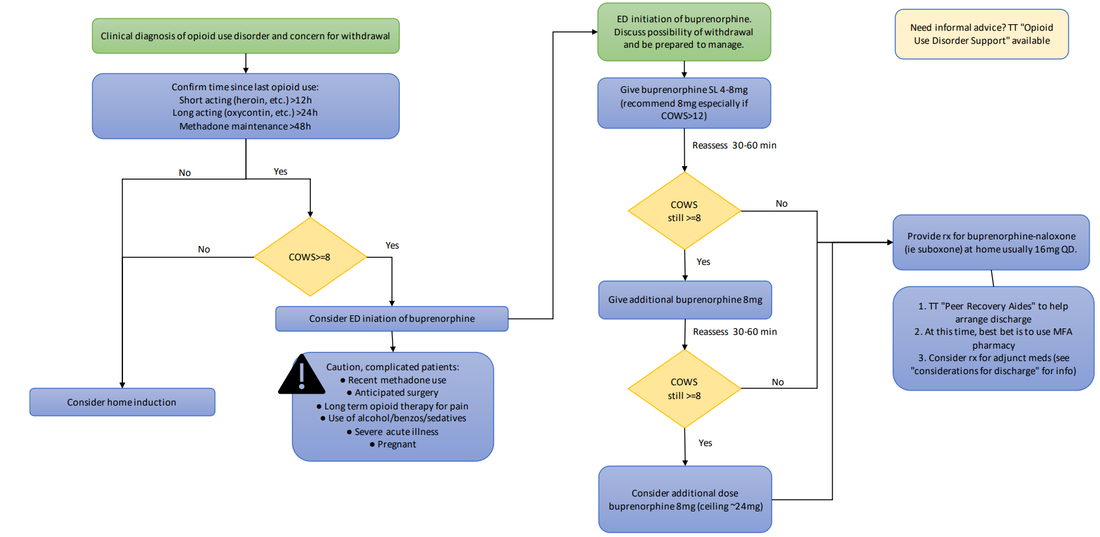
ED Flowchart
| PDF Version of ED Flowchart |
Adjunctive medications for treatment of opioid withdrawal symptoms
Withdrawal Symptoms |
Adjunctive Medications |
Anxiety/restlessness |
Clonidine 0.1mg, take 1 tab TID PRN sweats or palpitations (do not take if lightheaded), disp #6 Gabapentin 300mg, take 1 tab BID PRN restlessness, disp #4 |
Insomnia |
Trazodone 50mg, take 1 tab QHS PRN insomnia, disp #3 |
MSK pain |
Acetaminophen or ibuprofen |
Stomach cramps |
Dicyclomine 10-20mg q4h PRN stomach cramps, disp #12 |
Nausea/vomiting |
Ondansetron 4mg tab, take 1-2 tabs TID PRN nausea, disp #12 |
Diarrhea |
Loperamide 2mg tab, take 2 tabs once then 1 tab after each loose stool up to 6 times per day, disp #12 |
Patient Home Induction Handout for Discharge
| patient_home_induction_handout.pdf |
Considerations for Discharge
Want to talk to a provider for support?
a. “Opioid Use Disorder” Tiger Text Role. Informal support role regarding initiation (run by Dr. Catalanotti and Dr. Carbanera), M-F 8a-5p, support not consult
b. National Clinician Consultation Center Substance Use Warmline. M-F 6am-5pm. Voicemail 24 hours a day, 7 days a week. Specialty addiction medicine consultation (855) 300-3595
b. National Clinician Consultation Center Substance Use Warmline. M-F 6am-5pm. Voicemail 24 hours a day, 7 days a week. Specialty addiction medicine consultation (855) 300-3595
getting patient set up with MAT provideR
“Peer Recovery Aides” via TT can assist with getting patient set up with MAT provider. Ideally consult them early, so that by time of discharge they can have completed their assessment and possibly even have a follow-up appointment set up for the patient.
DC resources where there are MAT providers
If for some reason unable to do the above, here are some DC resources where there are MAT providers:
a. If someone is an MFA patient, or has insurance that MFA takes, DURING BUSINESS HOURS may TT Dr. Jill Catalanotti (cannot take Medicaid managed care); do not just refer to her though as often not taking patients
b. Peer Recovery Aide usually refers to DC- Medical Home Development Group 2112 F St NW Suite 504, Washington DC 20037. (202) 684-2784
c. Other clinics to consider, all of whom accept Medicaid Managed Care: Unity (East of the River), Whitman Walker, Bread for the City, Family and Medical Counseling Service (FMCS)
a. If someone is an MFA patient, or has insurance that MFA takes, DURING BUSINESS HOURS may TT Dr. Jill Catalanotti (cannot take Medicaid managed care); do not just refer to her though as often not taking patients
b. Peer Recovery Aide usually refers to DC- Medical Home Development Group 2112 F St NW Suite 504, Washington DC 20037. (202) 684-2784
c. Other clinics to consider, all of whom accept Medicaid Managed Care: Unity (East of the River), Whitman Walker, Bread for the City, Family and Medical Counseling Service (FMCS)
Pharmacy consideration as of May 2023
a. Locally there is still an issue with some pharmacies having an automatic system asking for X-waiver information. MFA pharmacy doesn’t have this so is probably the easiest place to get the rx sent to. Grubb pharmacy is also able to fill non-waivered prescriptions.
b. Ideally should talk with pharmacy to confirm they have the medication in stock and make sure the formulation (film vs tablet) you chose will be covered by patient’s insurance.
b. Ideally should talk with pharmacy to confirm they have the medication in stock and make sure the formulation (film vs tablet) you chose will be covered by patient’s insurance.
ED resources for buprenorphine initiatioN
CA Bridge: really comprehensive website
ACEP Buprenorphine use tool: Pretty simple “all you need to know” page, ED specific.
Providers Clinical Support System: more general information (not just ED specific)
ACEP Buprenorphine use tool: Pretty simple “all you need to know” page, ED specific.
Providers Clinical Support System: more general information (not just ED specific)