Head & Neck
Head, Negative Trauma
The head is atraumatic, without swelling or ecchymosis of the face or behind the ears, including the periorbital area. There is no tenderness to face, and the oral and nasal mucosa are nonbloody. Dentition is intact. The TMs are without hemotympanum
The head is atraumatic, without swelling or ecchymosis of the face or behind the ears, including the periorbital area. There is no tenderness to face, and the oral and nasal mucosa are nonbloody. Dentition is intact. The TMs are without hemotympanum
Head, Negative Medical
The head is normocephalic, without drainage from the eyes or nares. Sclera are white without injection or jaundice, and there is no rash or erythema of the face. External ears are without swelling, erythema, or tenderness. There is no pain or stiffness with neck range of motion.
The head is normocephalic, without drainage from the eyes or nares. Sclera are white without injection or jaundice, and there is no rash or erythema of the face. External ears are without swelling, erythema, or tenderness. There is no pain or stiffness with neck range of motion.
Neck, Negative Trauma
There is no midline cervical neck tenderness or stepoffs. The patient denies any numbness, tingling, or weakness of the extremities. The patient is able to range their neck completely without midline cervical pain, numbness, tingling, or weakness.
There is no midline cervical neck tenderness or stepoffs. The patient denies any numbness, tingling, or weakness of the extremities. The patient is able to range their neck completely without midline cervical pain, numbness, tingling, or weakness.
|
Spurling Test, Positive
The patient's head was turned to the affected side while extending and applying downward pressure to the top of the patient's head. Pain was elicited along a dermatomal pattern. |

|
Ophtho/ENT/Dental
Eyes, Fill-in
Bilateral eye examination showed _ periorbital swelling or ecchymosis, _ proptosis, and _ pain with EOM. The eyelids showed _ lacerations or ecchymosis. The sclera were white with_ chemosis or injection. Pupils were equal and reactive bilaterally, and extraocular muscles were intact. _ signs of chemical exposure or foreign body was identified, and there was _ peaked or teardrop pupil, enophthalmos, or obvious foreign body concerning for a potential globe rupture. Bilateral lids were everted without signs of foreign body. A fluorescein dye was instilled and under UV light no uptake was identified, and negative Seidel’s sign bilaterally. Intraocular pressures were _
Bilateral eye examination showed _ periorbital swelling or ecchymosis, _ proptosis, and _ pain with EOM. The eyelids showed _ lacerations or ecchymosis. The sclera were white with_ chemosis or injection. Pupils were equal and reactive bilaterally, and extraocular muscles were intact. _ signs of chemical exposure or foreign body was identified, and there was _ peaked or teardrop pupil, enophthalmos, or obvious foreign body concerning for a potential globe rupture. Bilateral lids were everted without signs of foreign body. A fluorescein dye was instilled and under UV light no uptake was identified, and negative Seidel’s sign bilaterally. Intraocular pressures were _
|
Ears
The bilateral tympanic membranes are non-erythematous without fluid level behind the membrane. External canals are normal, and there is no tenderness to the external ear or overlying the mastoid |

|
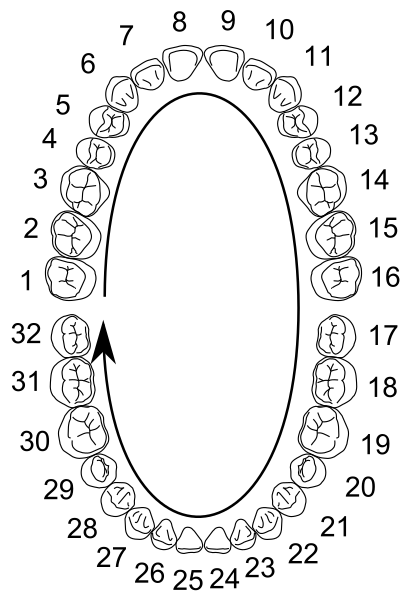
Teeth
|
Periodontal ligament injuries and features
|
Chest & Abdomen
Septic Re-eval
- Vital signs
- Cardiac
- Pulmonary
- Capillary refill
- Skin
- Peripheral pulses
Heart & Lung, Normal
No respiratory distress, lung sounds are clear bilaterally without wheezes, rhonchi, or rales. Heart rate and rhythm are regular, with normal S1S2 without murmur.
No respiratory distress, lung sounds are clear bilaterally without wheezes, rhonchi, or rales. Heart rate and rhythm are regular, with normal S1S2 without murmur.
Abdomen, Normal
The abdomen is soft, nontender, and nondistended, with _ surgical scars
The abdomen is soft, nontender, and nondistended, with _ surgical scars
GU
Female, Normal
A pelvic exam was performed with a female chaperone. The external genitalia was normal, without lesions. On speculum examination, the cervix was nonfriable and no blood was in the vaginal vault. On bimanual examination, there was no tenderness and no masses.
A pelvic exam was performed with a female chaperone. The external genitalia was normal, without lesions. On speculum examination, the cervix was nonfriable and no blood was in the vaginal vault. On bimanual examination, there was no tenderness and no masses.
Male, Normal
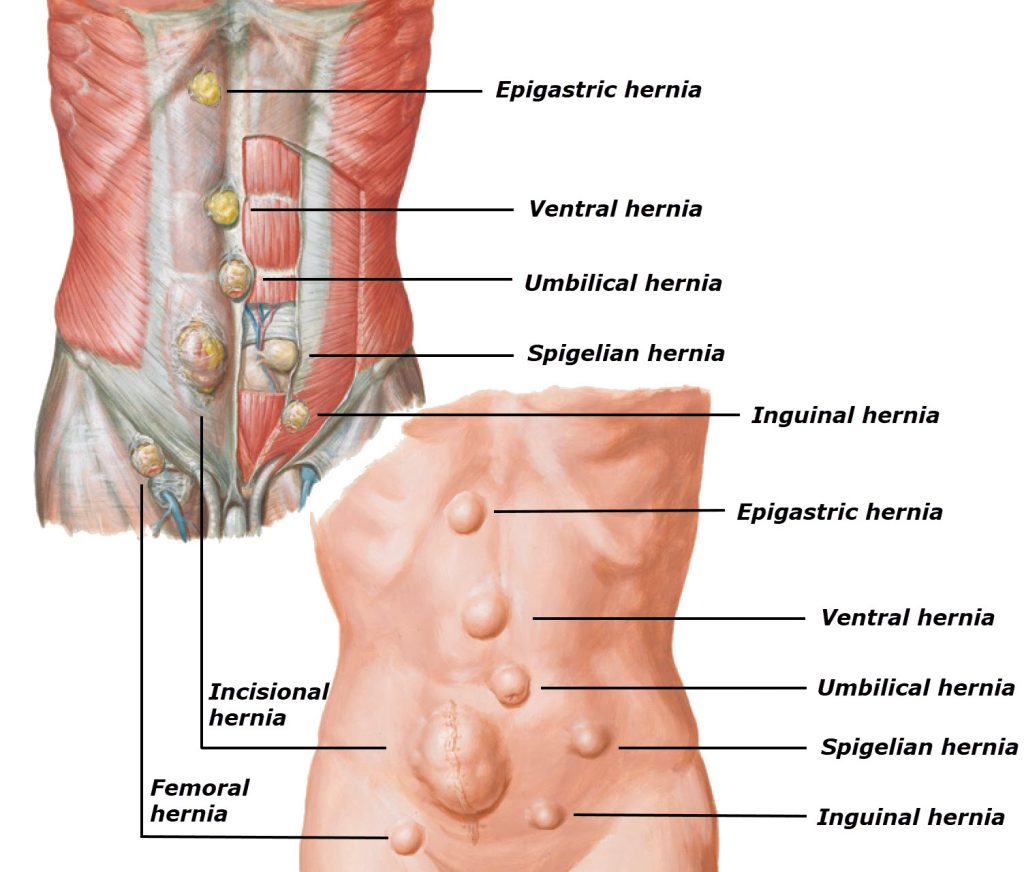
The external genitalia was normal, without lesions or ulcerations. There was no urethral discharge. The bilateral testicles were nontender without masses. No hernia bilaterally.
The external genitalia was normal, without lesions or ulcerations. There was no urethral discharge. The bilateral testicles were nontender without masses. No hernia bilaterally.
Indications for indwelling foley
The criteria for insertion and continuation of urinary catheterization in adults include:
H = Hematuria with clots/urethral trauma
O = Obstruction (retention/neurogenic bladder)
U = Urologic or other surgical procedure
I = Ins & Outs (strict measurement)
N = No code due to end of life care
I = Immobility
The criteria for insertion and continuation of urinary catheterization in adults include:
H = Hematuria with clots/urethral trauma
O = Obstruction (retention/neurogenic bladder)
U = Urologic or other surgical procedure
- GU surgery
- Prostate surgery
- Prolonged duration of surgery (>4 hrs.)
- Large volume infusions
- Diuretics during surgery
- Intra‐operative monitoring of urinary output
I = Ins & Outs (strict measurement)
N = No code due to end of life care
I = Immobility
- Unstable fractures (trauma patients)
- Balloon Pump
- Epidural anesthesia
- Intracranial Pressure Issues
- Other: Must Have Documented Reason
Extremities & Back
|
Shoulder, Trauma Fill-in
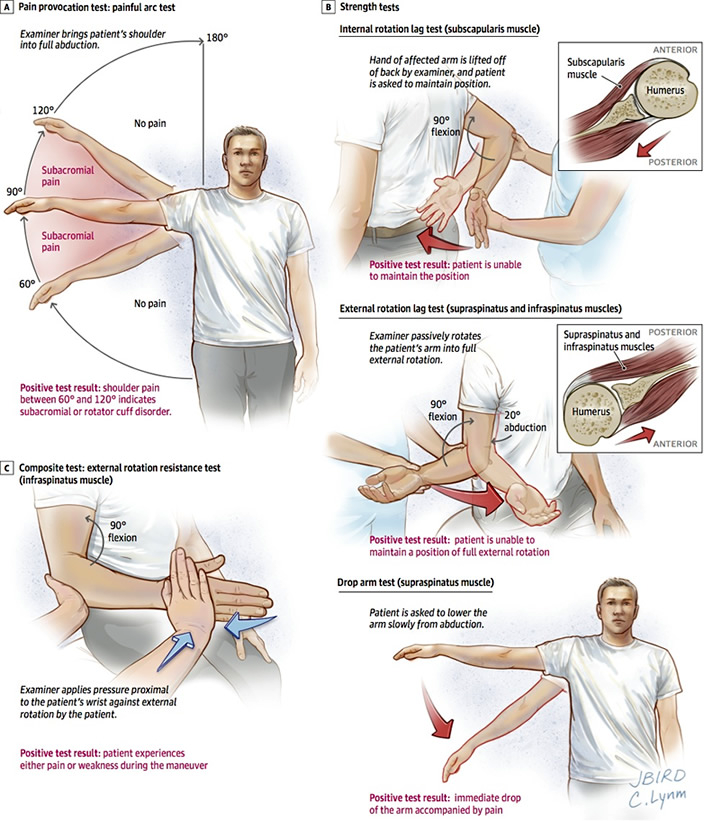
Inspection of _ shoulder shows _ lacerations, _ discoloration, and _ swelling or deformity. The clavicle is nontender without deformity. Palpation of the shoulder reveals _tenderness. There is _ sensation along the lateral deltoid. The rotator cuff musculature was tested, revealing _. |
|
|
Hand, Trauma Fill-in
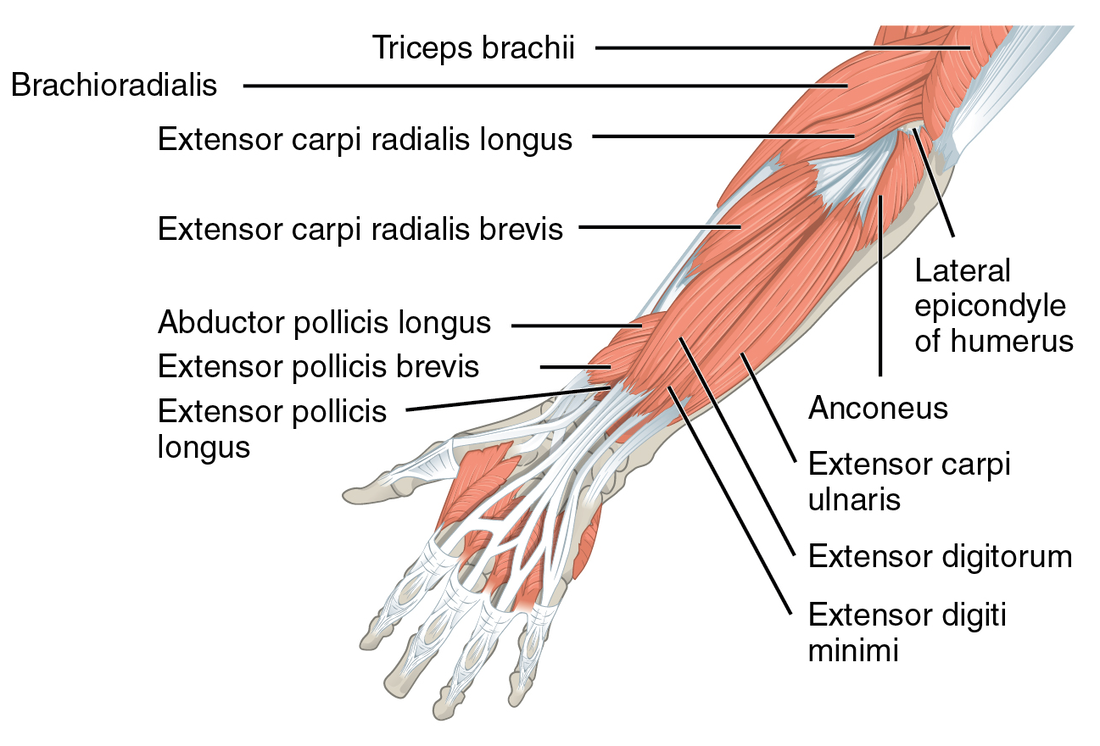
Inspection of _ hand shows _ lacerations, _ discoloration, and _ swelling or deformity. Palpation reveals _tenderness. The median nerve was tested at the IP joint for Flexor Pollicus Longus, and at the second DIP joint for Flexor Digitorum Profundus. The Thenar muscles were tested for resistance to dorsal and palmar thumb movements, and the Abductor Pollicus Brevis was palpated during contraction. The Ulnar nerve was tested at the interosseous muscles with resistance to adduction of the phalanges. Froment’s Sign was tested at the radial aspect of the second digit and the thumb and _normal. The Radial nerve was tested with individual phalange extension. DIP and MIP flexion was tested in isolation with each digit. During testing of the flexor and extensor tendons, _ pain was elicited along the tendon pathways. Hand, Simple
Extension intact throughout. 3rd digit. Sensation intact over the pad of the finger, thenar eminence, into webspace between 1st and 2nd finger. Patient able to spread fingers to resistance, extend wrist to resistance, patent oppose 1st and 2nd finger to resistance. |

|
Back Pain, Normal
The thoracic and lumbar back was examined, there are no surgical scars, there is no rashes, ecchymosis, or swelling. There is no midline step-offs or midline tenderness. The patient has negative straight leg raise and negative cross leg raise bilaterally. The patient has intact strength in the bilateral lower extremities. The patient does have tenderness to palpation along the _.
The thoracic and lumbar back was examined, there are no surgical scars, there is no rashes, ecchymosis, or swelling. There is no midline step-offs or midline tenderness. The patient has negative straight leg raise and negative cross leg raise bilaterally. The patient has intact strength in the bilateral lower extremities. The patient does have tenderness to palpation along the _.
Knee, Trauma Fill-in
The bilateral lower extremities were examined. There was tenderness to the _. There were no skin changes, including ecchymosis, abrasions, lacerations, or lesions. The bilateral knees had normal anterior and posterior drawer tests, and normal Valgus and Varus strain. There was no tenderness to the bilateral patella, and _ joint effusion. The patient
was _ to extend each knee fully.
The bilateral lower extremities were examined. There was tenderness to the _. There were no skin changes, including ecchymosis, abrasions, lacerations, or lesions. The bilateral knees had normal anterior and posterior drawer tests, and normal Valgus and Varus strain. There was no tenderness to the bilateral patella, and _ joint effusion. The patient
was _ to extend each knee fully.
Leg, DVT Exam
The bilateral lower extremities have no edema, calves are nontender, and no pain with ankle ROM. No skin lesions. Pulse, motor, and sensory are intact. At 10cm below the tibial tuberosity, the legs are _ in diameter
The bilateral lower extremities have no edema, calves are nontender, and no pain with ankle ROM. No skin lesions. Pulse, motor, and sensory are intact. At 10cm below the tibial tuberosity, the legs are _ in diameter
Ankle, Ottowa Fill-in
The _ ankle appeared _ atraumatic without swelling ecchymosis, or abrasions. There was _ tenderness to the posterior medial and lateral malleolus. There was _ tenderness overlying the 5th metatarsal. There was _ midfoot tenderness. Brisk cap refill was present, and sensation was intact along the lateral aspect of the foot as well as the first and second digits.
The _ ankle appeared _ atraumatic without swelling ecchymosis, or abrasions. There was _ tenderness to the posterior medial and lateral malleolus. There was _ tenderness overlying the 5th metatarsal. There was _ midfoot tenderness. Brisk cap refill was present, and sensation was intact along the lateral aspect of the foot as well as the first and second digits.
Skin
| fundamentals-of-dermatology.pdf |
|
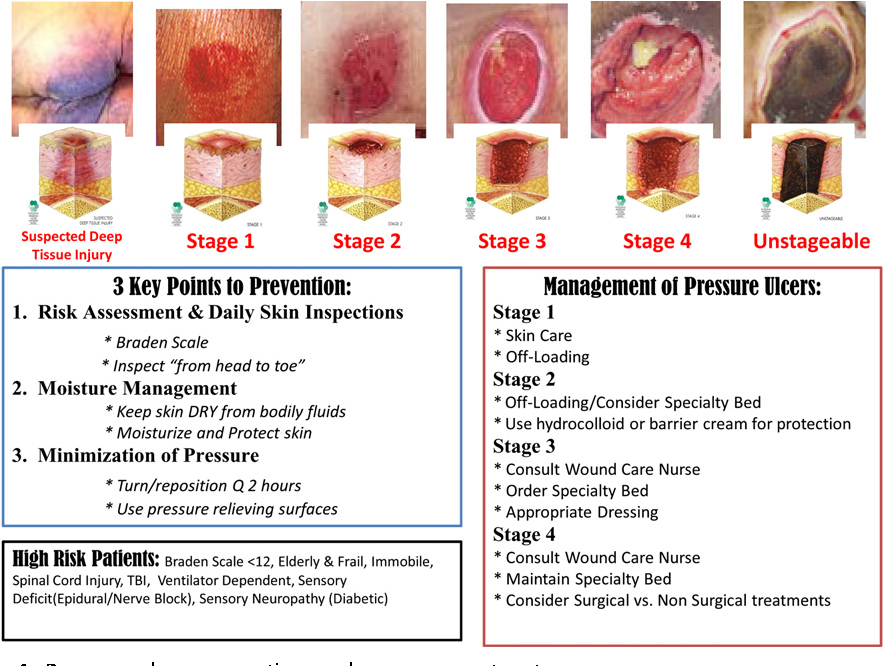
Pressure Ulcer Staging
|
|
Neuro
|
Normal Real-world Neuro
The patient's vision is grossly normal including visual fields. EOMI. No facial droop or tongue deviation. Speech intact without slurring. No word-finding difficulty. Strength in all four extremities 5/5, and sensation was intact in all extremities. Normal rapid hand movements and normal finger-nose coordination. Romberg test negative and gait intact, including heel-toe. The patient is able to follow commands with right-left orientation. |
Normal Full Neuro
Cranial nerves 2-12 were tested and intact. Extraocular muscles intact, without any nystagmus. Strength in all four extremities was 5/5, and sensation was intact in all extremities. The patient had normal rapid hand movements and normal finger-nose coordination. Romberg test negative, and gait intact, including heel-toe.
Cranial nerves 2-12 were tested and intact. Extraocular muscles intact, without any nystagmus. Strength in all four extremities was 5/5, and sensation was intact in all extremities. The patient had normal rapid hand movements and normal finger-nose coordination. Romberg test negative, and gait intact, including heel-toe.
Functional quadriplegia
(or quadriparesis) is defined as the complete inability to move due to severe disability or frailty caused by another medical condition without physical injury or damage to the brain or spinal cord.
(or quadriparesis) is defined as the complete inability to move due to severe disability or frailty caused by another medical condition without physical injury or damage to the brain or spinal cord.