|
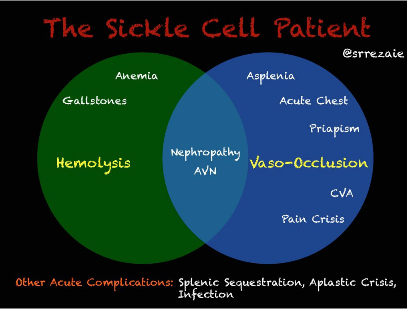
Adapted from Colton Hood's August 17th 2016 Grand Rounds lecture. One of the most common and severe complications of sickle cell disease, clinically may resemble a pneumonia, and can develop suddenly, and is more common in patients with asthma or those with prior acute chest events. Typically presents with cough, shortness of breath, and rales accompanied by a new infiltrate on chest X-ray. Mortality of acute chest syndrome is 9% in adults, and can lead to pulmonary hypertension, right heart failure, and risk of sudden death. 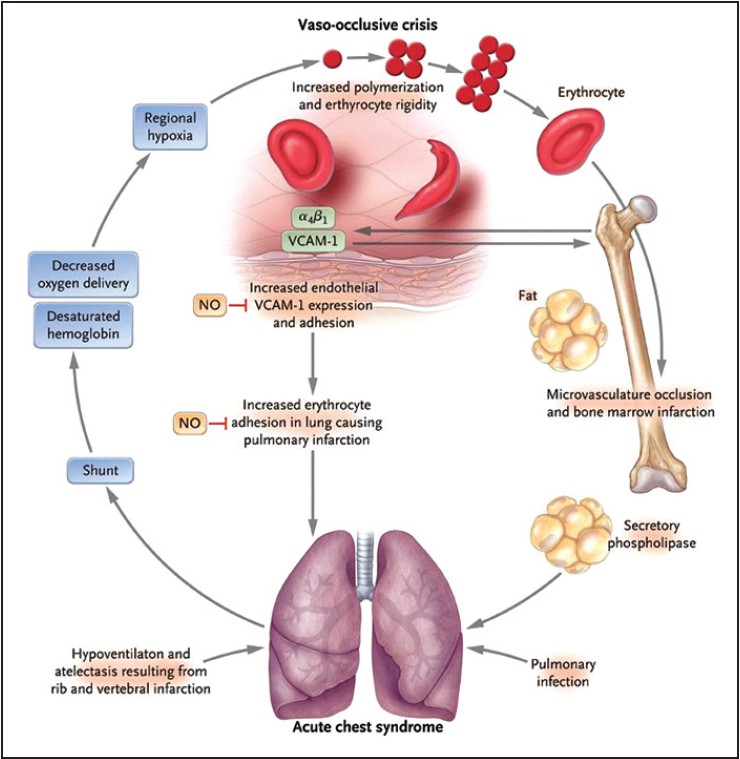 Source: http://www.ssajm.org/text.asp?2014/1/3/111/138930 Evaluate patients with sickle cell disease with acute onset of lower respiratory tract disease with or without fever for acute chest syndrome, including chest x-ray and pulse oximetry to measure oxygen saturation (NHLBI Consensus-Panel Expertise)
1 Comment
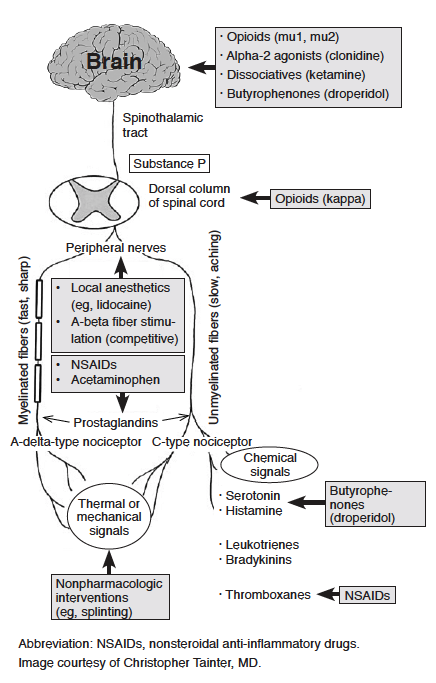
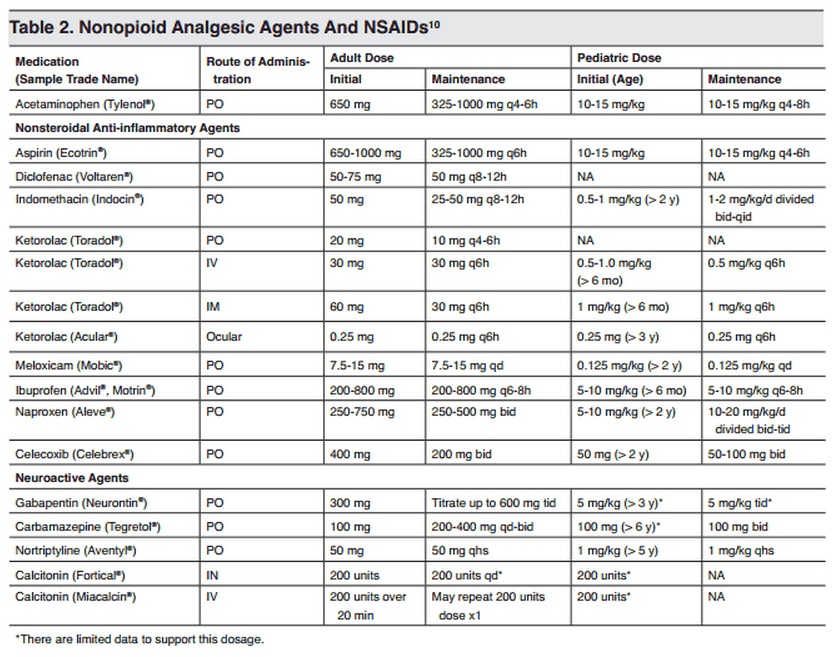
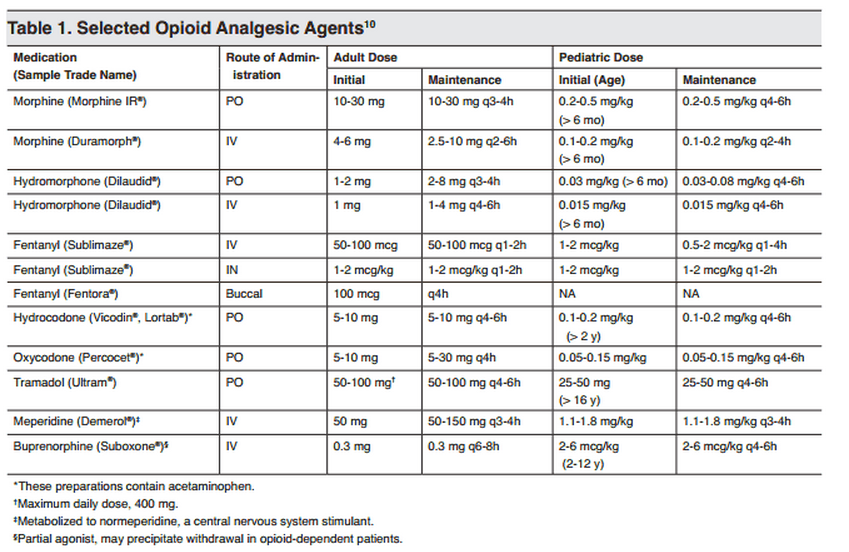
Adapted from Dr. Doberman's Principles of Analgesia, Palliative & Geriatrics Make sure you are appropriately treating your patient's pain! Use the appropriate dosages at the appropriate intervals; PO medications should be redosed every 3-4 hours for short-acting medications. IV opioids should be redosed every 1-2 hours. Titrate your dosing to patient comfort. In severe pain, titrate rapidly with short acting opioids, and change to longer acting medications when pain relief is achieved. During in-patient services, always remember to provide a breath through pain medication that provides 10-20% of their normal 24 hour oral dose, or 50-100% of their hourly IV rate. 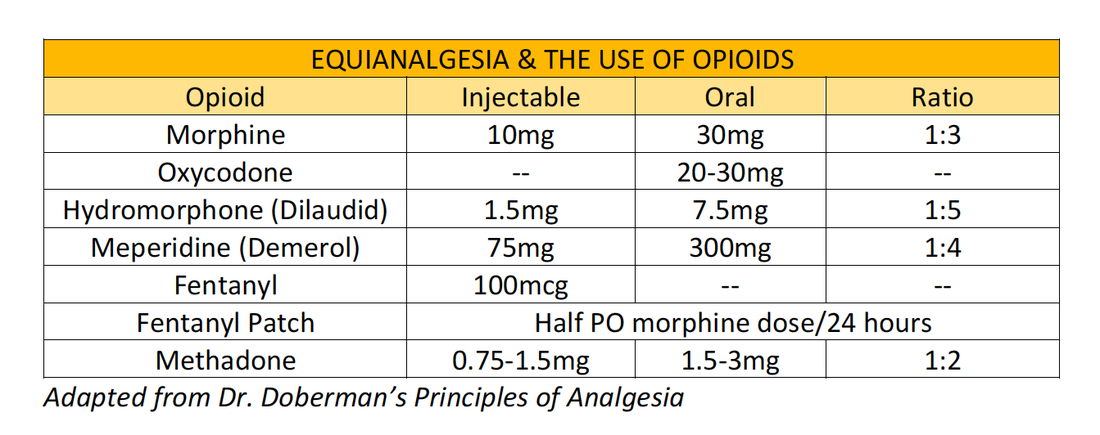
Naproxen With Cyclobenzaprine, Oxycodone/Acetaminophen, or Placebo for Treating Acute Low Back Pain1/6/2016 According to this new article from JAMA, the addition of Percocet or Flexeril to Naproxen does not improve functional outcomes in acute low back pain. The article compared functional outcomes in lower back pain at 1 and 3 weeks between Naproxen, Flexeril, and Percocet. Via a randomized, double-blind study in NYC, 323 patients were randomized to Naproxen + Placebo, Naproxen + Flexeril, and Naproxen + Percocet. Using an improvement in the Roland-Morris Disability Questionnaire (RMDQ), the study found that adding cyclobenzaprine or oxycodone/acetaminophen to naproxen alone did not improve functional outcomes or pain at 1-week follow-up. These findings do not support use of these additional medications in this setting.
|
Categories
Archive
February 2018

Please read our Terms of Use.
|