|
61 year old presents to the ED with chest pain radiating to his shoulder 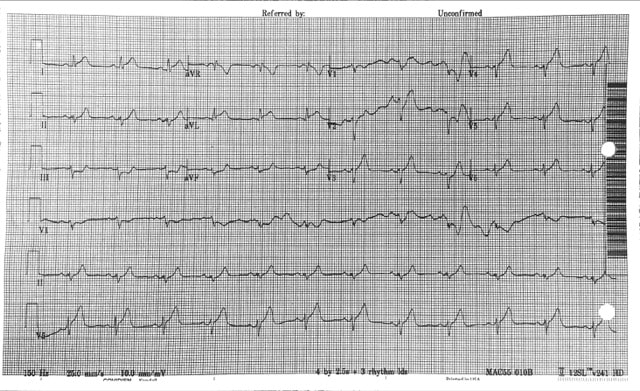 What is the diagnosis?
Anterior STEMI
Elevations of the ST segments in the precordial leads. There are ST depressions (reciprocal changes) inferiorly (Green arrows), poor R wave progression (Red) and T waves that are more symmetric (yellow). Additionally the patient is 61 years old. 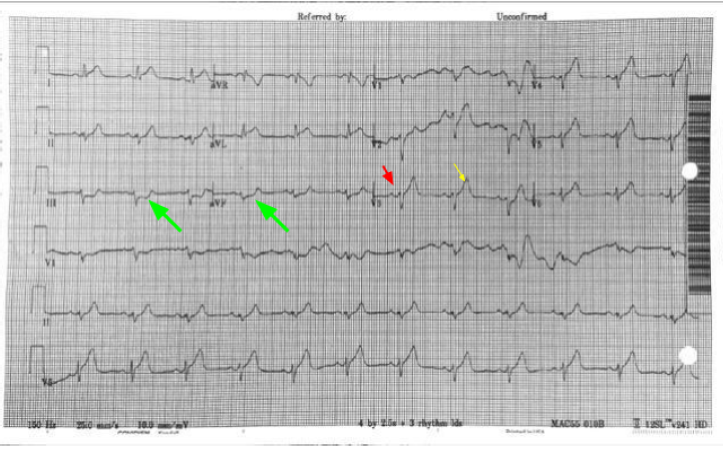
Why Not...
Why is this not Benign Early Repolarization?
The differentiation of benign ST elevations (BER) and Anterior STEMI can be difficult. There are a number of characteristics which are suggestive of BER vs. STEMI. Make sure to examine for other ischemic changes. Our job is to exclude MI and BER should be diagnosis of exclusion. Some features suggestive of each in below table. 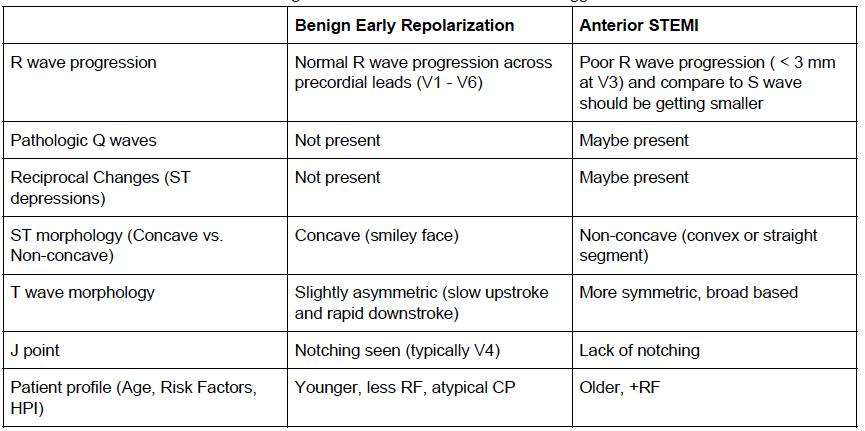
Learn more
Consider using the Subtle Anterior STEMI calculator in cases where you are concerned, but the EKG may be difficult to decipher
0 Comments
Since October 20th, 2017, an increased number of mumps cases in college students have been reported from DC Universities. Mumps is an acute viral disease caused by a paramyxovirus. Symptoms include fever and swelling of unilateral or bilateral parotid or other salivary glands. Swelling usually peaks in 1 to 3 days, and can last 2 or more days before subsiding. In approximately one-third of cases, mumps infection may present with nonspecific or primarily respiratory symptoms, and can also be subclinical. A person with mumps is generally contagious two days before onset of symptoms to 5 days after. The incubation period is 14-18 days from the time of exposure, but can be as long as 25 days. Mumps spreads from person to person via respiratory secretions or saliva or through fomites. Diagnostic Testing Please obtain the following specimens as soon as mumps is suspected: · Oral or buccal swab samples. Massage the parotid gland for 30 seconds and store in 2 ml of viral transport medium. Refrigerate samples at 4°C for shipment within 24 hours and ship on cold packs (store at -70°C if delayed). · Serum in a red-top or serum separator tube for IgG and IgM testing Detailed specimen collection instructions can be found on the CDC website (https://www.cdc.gov/mumps/lab/specimen-collect.html). It is critical to perform mumps PCR for confirming the diagnosis as serology test result can be misleading especially in previously vaccinated persons. For additional questions regarding specimen collection, please email [email protected]. Reporting Cases to DOH Suspected cases of mumps infection should be reported IMMEDIATELY to the Department of Health at (202)-442-9371 or via the DC Reporting and Surveillance Center (DCRC) on our Infectious Disease website (https://doh.dc.gov/service/infectious-diseases). Reports should be made at time of initial clinical suspicion of mumps infection. If diagnosis of mumps is considered and diagnostic testing are ordered, the case should be reported at that time. Do not wait for laboratory confirmation. Vaccination Updated guidelines from the Advisory Committee on Immunization Practices (ACIP) indicate that a 3rd dose can be recommended in outbreak settings for identified high-risk groups. Healthcare providers can consult with DC DOH to determine whether an additional vaccine dose is indicated. A fact sheet on (https://doh.dc.gov/page/disease-fact-sheets). Please contact the DC DOH Division of Epidemiology–Disease Surveillance and Investigation at: Phone: 202-442-8141(8:15am-4:45pm) | 844-493-2652 (after-hours calls) Fax: 202-442-8060 | Email: [email protected]
|
Categories
Archive
February 2018

Please read our Terms of Use.
|
||