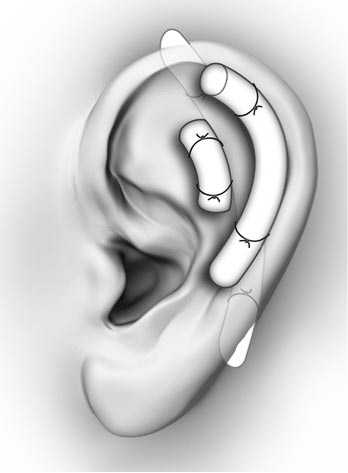
Auricular Hematoma
Otitis ExternaOtitis externa is frequently caused both by swimmer and water exposure as well as the use of household items to 'clean out' the ear. This should be treated with cipro otic drops, and patients should not be placed on oral antibiotics as this will only increase the risk for fungal infection and not assist in treating the bacterial infection. Consider placing an ear wick to help increase the amount of antibiotic which reaches the infected area. Bullous MyringitisAn infection of the ear drum that causes severe pain and loss of hearing. On examination a red or clear blister will be present on the ear drum. Treatment is antibiotics and rupturing the blister. Tympanic Membrane PerforationsTypically due to blunt trauma or direct penetrating trauma from Q-tips or other objects. Ciprodex antibiotic drops, and water precautions should be given, as well as ENT followup. Those with severe symptoms such as hearing loss, vertigo, or nystagmus should have urgent ENT followup. Otitis MediaOver 70% of OM is viral, but it is difficult to determine viral vs bacterial. Most bacterial infections are strep pneumo (50%). On exam the patient will have bulging of the TM or an air-fluid level. To accurately diagnose OM, you should be unable to move the TM with suction. Treatment is to either wait and watch or provide high-dose amoxicillin. Sudden Sensorineural Hearing LossAcute loss of hearing without an external or conductive cause. It is sudden (<72 hours) and unilateral, caused by viral, ischemic, or auto-immune causes. Syphilis and idiopathic intracranial hypertension can both cause acute unilateral hearing loss. Many cases are idiopathic. Treatment is either PO steroids or direct steroids to the middle ear, and urgent ENT followup. Antivirals should only be given if there are signs of a vesicular lesion. Bell's PalsyPatients presenting with symptoms of Bells Palsy should have a full history and physical examination to identify facial paralysis and possible causes, including evaluated for lesions of the TM concerning for Ramsay Hunt Syndrome. The AAO do not recommend routine lab testing or imaging in patients with Bell's Palsy, unless the patient lives in an area with endemic Lyme Disease. Patients should be treated with both oral antiviral AND oral steroid treatment together within 72 hours of symptom onset. Antiviral treatment alone is not recommended, however steroids alone may still have benefit. Patients should be sent home with eye protection and eye drops to prevent trauma and corneal abrasions or ulcers. AAO Guidelines.
0 Comments
Leave a Reply. |
Categories
Archive
February 2018

Please read our Terms of Use.
|