|
Adapted from Pouya Gharahdaghi's Grand Rounds Lecture, September 7th, 2016 A discussion of acute liver disease, hepatitis, hepatic encephalopathy and coagulopathies and complications of liver disease Viral HepatitisHepatitis B: Frequently sexually transmitted or parental transmission. Usually vaccinated for in the US. If exposed to Hepatitis B blood, ensure the patient is appropriately vaccinated. If they are not appropriately vaccinated, then the patient should receive HBIG as well as the Hep B vaccine at 0, 1, and 6 months. Hepatitis C: Frequently transmitted by IV drug use, asymptomatic in most initially infections, however 75% will progress to chronic hepatitis. Hepatitis E: Associated with Hep B and results in fulminant hepatitis. Toxic HepatitisAcetaminophen: Causes 40% of liver failure
Medications Amantia & Phalloides mushrooms Chronic Hepatitis and CirrhosisCirrhosis becomes symptomatic when 80% of the liver is damaged & cirrhotic. Symptoms will frequently include esophageal varicies, ascities, hemorrhoids. Further evaluation for liver disease complications includes abdominal ultrasound, chest X-ray, and laboratory evaluation. Spontaneous Bacterial PeritonitisIdentification of SBP by paracentesis requires 30-40cc of ascites. Lab evaluation should include;
Hepatic Encephalopathy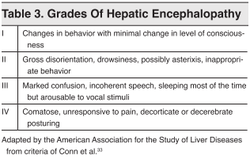 A diagnosis of exclusion, seen with chronic liver failure due to failure of the liver to process ammonia. Although an ammonia level is useful in acute failure, ammonia levels are less useful for trending in chronic liver failure. Normally, ammonia is converted to Urea and removed by the GI tract. When ammonia is elevated, it is modified to glutamine, which crosses the blood-brain-barrier causing swelling and altered mental status. Treatment is lactulose by naso-gastric tube if altered and unable to take PO, or rectally. This can be combined with Rifaximin to increase the rate of resolution and mortality.
0 Comments
Leave a Reply. |
Categories
Archive
February 2018

Please read our Terms of Use.
|
||