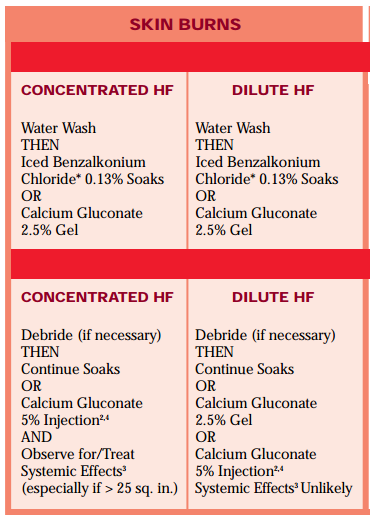
Burns of dilute hydrofluoric acid are difficult to distinguish from other chemical burns and can appear as minimally erythematous areas of skin without blistering. Over 12-24 hours, however, this can progress to severe burns and blistering, progressing to necrosis requiring debridement. Highly concentrated acids may present with severely reddened, swollen areas with blanched regions which rapidly progress to necrosis. Even burns without impressive physical appearance may cause severe pain due to nerve ending irritation. HF is unique in that it does not spontaneously dissociate from hydrogen ions, causing it to penetrate through the skin and cause deeper, even systemic damage and hypocalcemia and hypomagnesemia. Hydrofluoric acid burns of 1% with industrial strength HF can be enough to cause fatal hypocalcemia. With industrial strength HF, there are immediate effects, while lower concentration burns can cause minimal acute onset with effects beginning in 12-24 hours. Inhalation damage is rare, but can occur with solutions with large amounts of HFA. Concomitant exposures are atypical, however other strong acids may be found in mixtures with HF. PresentationAs hydrofluoric acid absorbs into the skin, the fluoride binds irreversibly to the calcium and magnesium, causing hypocalcemia and hypomagnesia. Systemic effects of hypocalcemia and hypomagnesia will result in hypotension, prolonged QT and bradycardia. Burns may not appear severe despite systemic symptoms. Progressive bradycardia and tetany with eventual cardiac arrest. Theoretically, hyperkalemia is caused secondary to hypocalcemia, however many cases have no potassium derangement. Skin Burn TreatmentAfter immediate decontamination, begin soaking the tissue in 0.13% benzalkonium, which is frequently started on scene. 2.5% calcium gluconate gel should be applied frequently and massaged into the area until pain and erythema is resolved. with high concentration burns or large BSA, Local injections of 5% calcium gluconate is indicated for larger burns, or when gel does not provide relief within 30-40 minutes. Calcium chloride is contraindicated, as this is corrosive to local tissue. If nailbeds are involved, the recommended treatment is to remove the nail for surface treatment. Intra-arterial and intravenous calcium infusions may be required, and should be used in conjunction with poison control or burn center recommendations. Relief of pain is an excellent indication of treatment success, so local anesthetics should be avoided.
0 Comments
Leave a Reply. |
Categories
Archive
February 2018

Please read our Terms of Use.
|
||||