Sickle Cell Disease - by Adbulla Genotypes
Pathophysiology
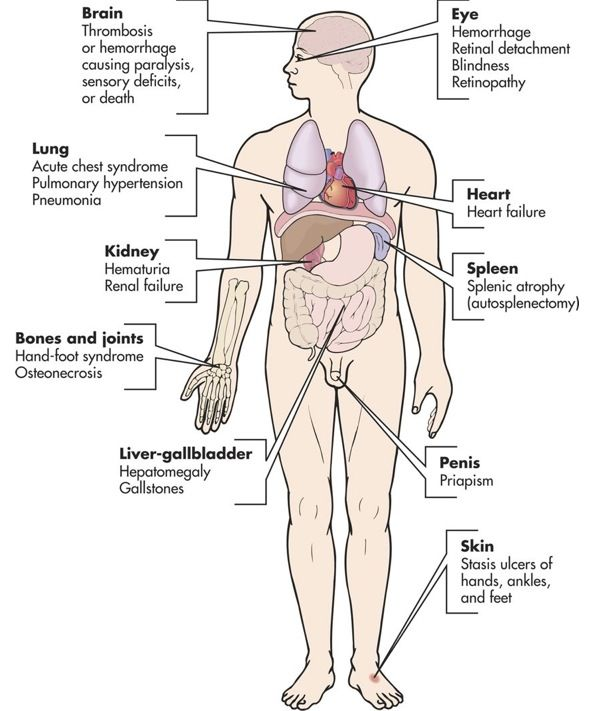
Clinical Manifestations
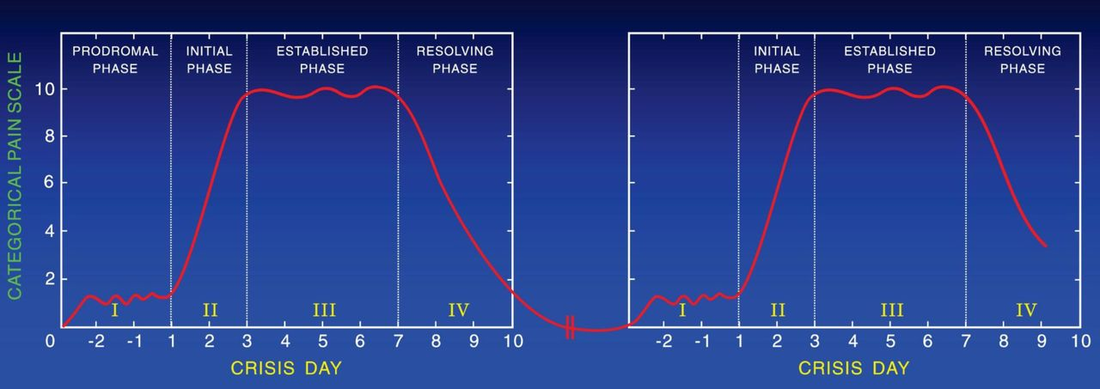
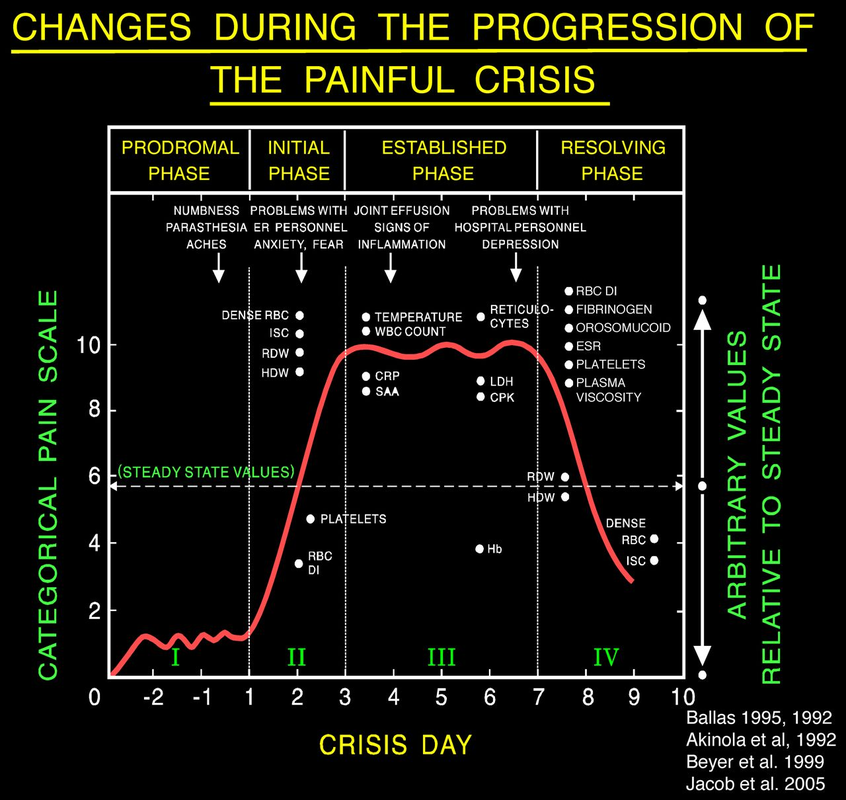 Vaso-occlusion
 Pts are often still d/c'd with pain, but ideally can handle it at home with PO pain meds 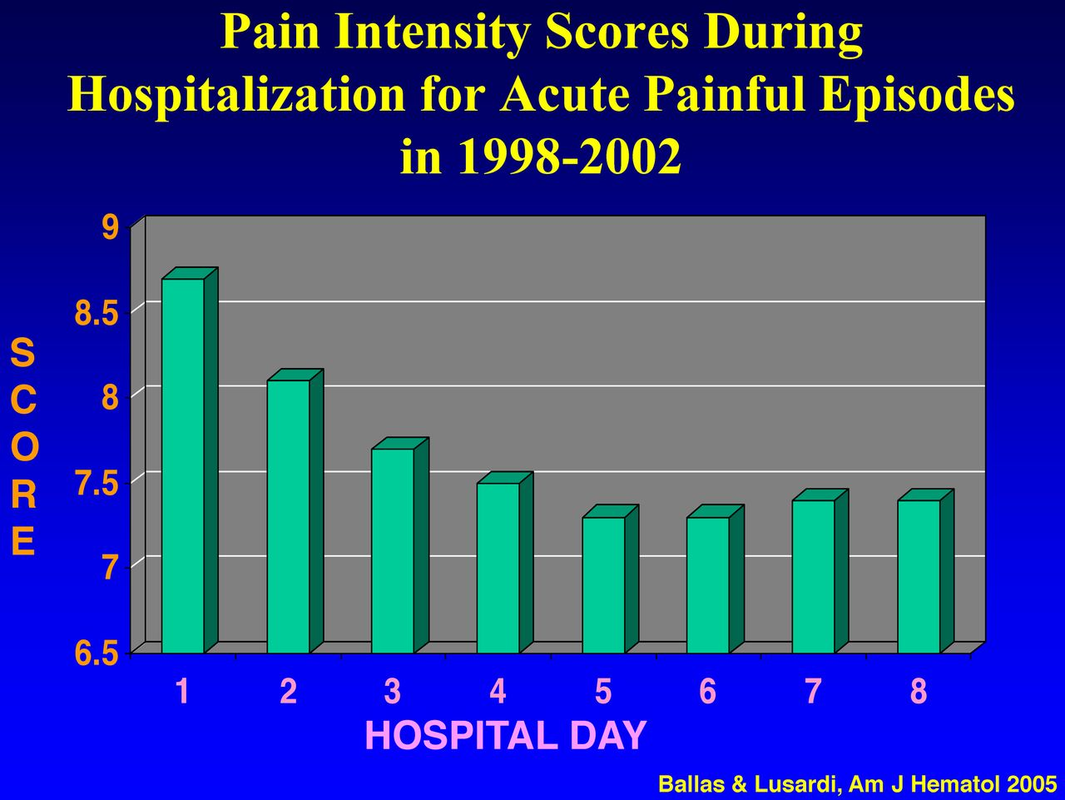 History
Physical Exam
 Labs
Pain Treatment
Hydration
Oxygen
Magnesium
TR Project: Pelvic Kits - by Colton Notes on doing a TR project:
Plan:
Pelvic Kit
Logistics
Study
Resources for TR Projects
 M&M Conference - by M-E Case:
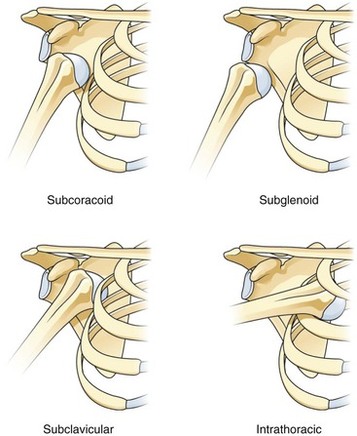
Shoulder Dislocation:
Chronic Shoulder Dislocations
0 Comments
Leave a Reply. |
Categories
Archive
February 2018

Please read our Terms of Use.
|