GU/Renal Board Review – by Stefanie Gilbert
 Ring Down Ring Down
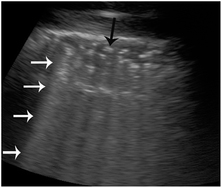
Ultrasound: Air Where it Shouldn’t Be – by Sean Chester
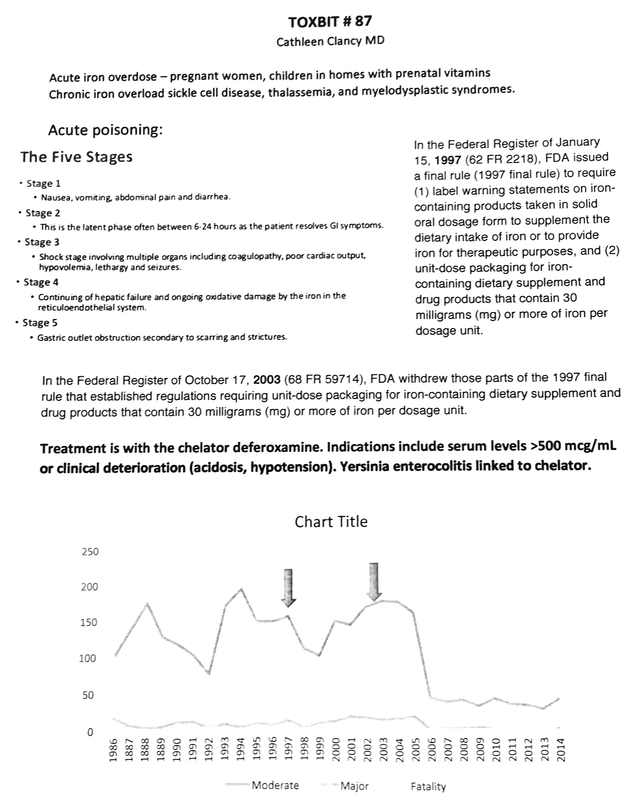 Tox Bit – by Dr. Clancy
Contrast-Induced Nephropathy – by Aziz Almehlisi
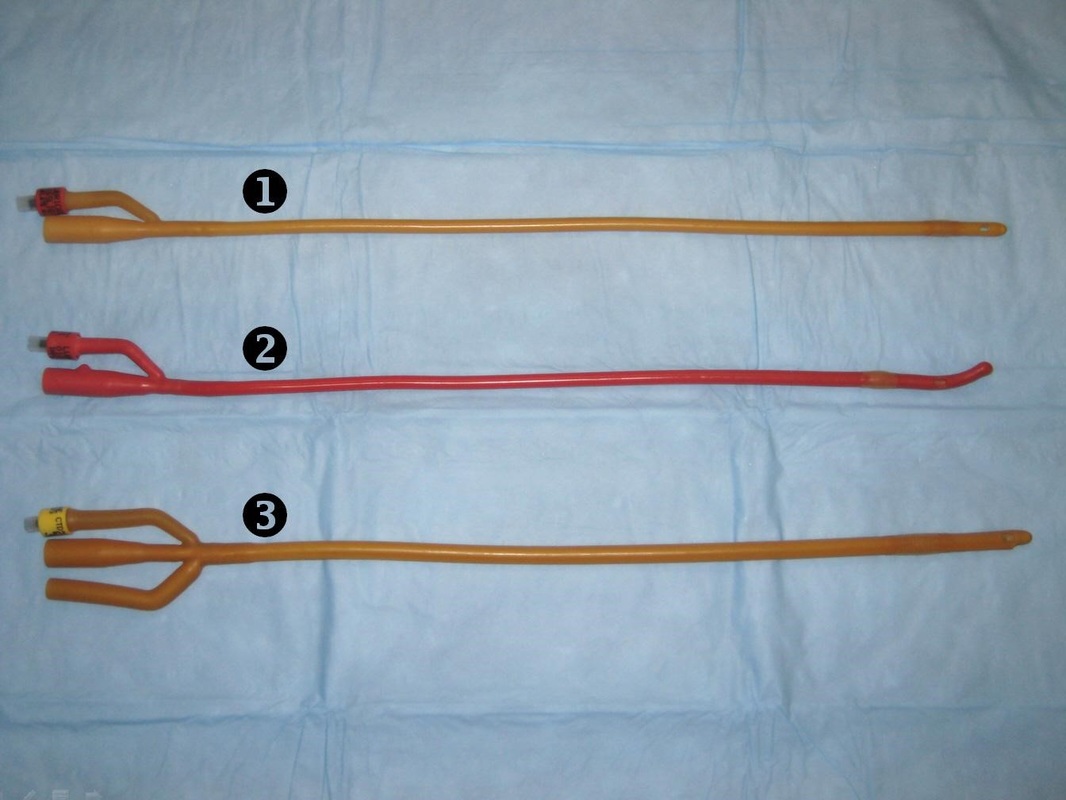
Specialty Conference: Acute Urinary Retention (AUR) – by Raj Gadhia with guest speaker Alice Semerjian (urology PGY-5)
King of the Hill: Legislation for Dummies – by Todd Clark
0 Comments
Leave a Reply. |
Categories
Archive
February 2018

Please read our Terms of Use.
|