|
Adapted from Dr. Calabrese's October 12th Grand Rounds presentation. 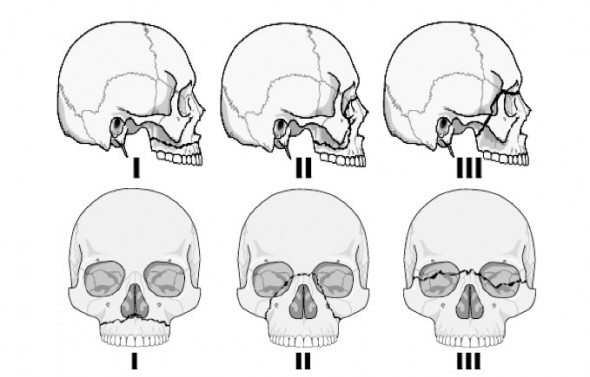 Evaluation of every facial trauma patient should include a complete facial assessment
Evaluation of the patient with Facial TraumaPatients presenting with facial trauma have several immediate concerns
Agitation can be due to pain, intoxication, or air hunger/airway compromise. It is important to not only recognize agitation but attempt to identify the cause. Your secondary survey must evaluate for skull and facial fractures, neurological injuries, and insidious airway injuries.
Orbital Injury & EntrapmentEvaluation of orbital fractures is important to identify entrapment of the extra-ocular muscles. Patients who have extra-ocular muscles require emergent ophthalmology consults if they have afferent pupilary defects or increased pressure, concerning for retrobulbar hematomas or nerve impact. A very subtle orbital floor fracture may present as a slight difference in the level of the pupils. Lateral Canthotomy IndicationsSuspected acute orbital compartment syndrome (OCS), plus one or more of the following:
Nasal InjuryEvaluate all your facial trauma patients for septal hematomas, nasal fractures and dislocations, and telecanthis (flattening of the nasal bridge). Telecanthis can indicate a higher potential for CSF leakage, and these patients will require further monitoring. Septal Hematomas can lead to;
Mandibular InjuryEvaluate not only the external mandible, but also the oral floor to evaluate for hematoma or expanding mass. Mandibular fractures can lead to airway compromise by deformation of the airway or tongue displacement. Lefort Fractures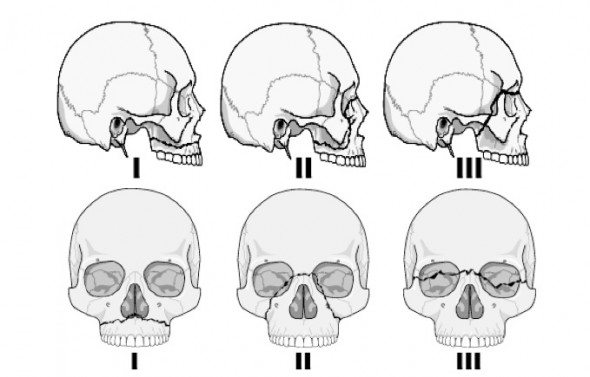 Patients with an initial evaluation concerning for a 'flattened' appearance to the face or significant trauma should have a higher suspicion of maxillary fractures leading to one of three Lefort fractures.
0 Comments
Leave a Reply. |
Categories
Archive
February 2018

Please read our Terms of Use.
|