|
45 M presents to the ED with lightheadedness after his LVAD “Low Flow” alarm sounded. He has a normal mental status, and MAP ~ 65 mmhg 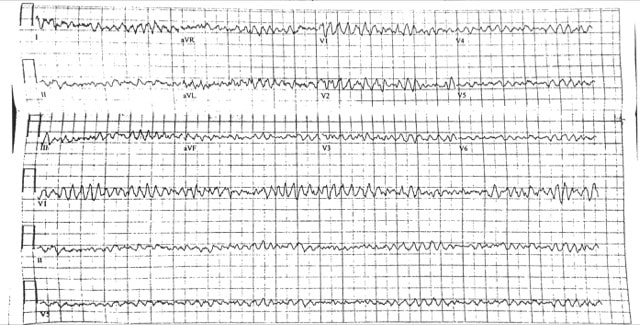 What is the rhythm?
Ventricular Fibrillation. There are no P waves nor organized QRS complexes. This distinction between coarse and fine V Fib is irrelevant. In theory fine V Fib indicates it has been a longer duration but management is not different. You may look at the EKG and question whether the patient has Torsades. The initial distinction is irrelevant as the patient is likely unstable / pulseless and needs electricity. Torsades can only be diagnosed with prolonged QT on the patient’s preceding or ensuing EKG. How would you typically manage this rhythm?
ACLS approach to tachycardias:
1.Does the patient have a pulse? 2. Shockable rhythm or not? If Pulse and unstable → Synchronized cardioversion (the electricity is timed to the cardiac cycle). If the patient is pulseless then analyze the rhythm and determine is it “Shockable” (Pulseless VTach or VFib) or “Non-shockable” (PEA or Asystole). The first step is immediate CPR in both scenarios until you can get the defibrillator to defibrillate the shockable rhythms (electricity not timed to cardiac cycle). ****THESE ARE THE PATIENTS THAT ACLS SAVES**** 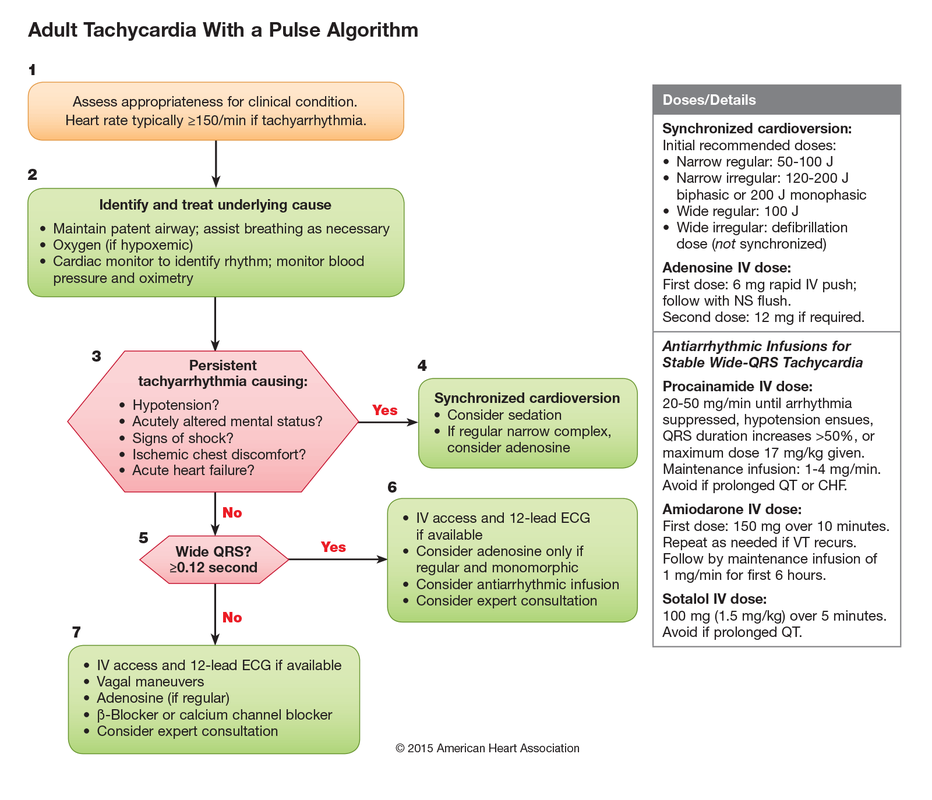
How would you manage this rhythm in lvad patients?
Call for help when they hit the door. You should NOT perform CPR in an LVAD patient unless you can confirm they are in cardiac arrest. Most often the pump needs troubleshooting. Arrhythmias are not uncommon. You can attempt chemical cardioversion (amiodarone) or electrical cardioversion. Pads do NOT go over the LVAD. Use the anterior/posterior positions.
Take Home Points 1. It is not important to distinguish between types of VFib → the answer is defibrillation 2. Torsades de Pointes can only be diagnosed if the preceding/ensuing EKG has prolonged QT 3. Do NOT perform CPR on LVADs unless Cardiac Arrest confirmed (eg MAP 0 mmHg) 4. When performing defibrillation or cardioversion in LVAD patients place pads Anterior / Posterior Resources: Partyka C and Taylor B. Review article: ventricular assist devices in the emergency department. Emerg Med Australas. 2014 Apr; 26(2): 104-12. Link MS, Berkow LC, Kudenchuk PJ et al. Part 7: Adult Advanced Cardiovascular Life Support: 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2015; 132:S444
0 Comments
Leave a Reply. |
Categories
Archive
February 2018

Please read our Terms of Use.
|