 What is the differential diagnosis?
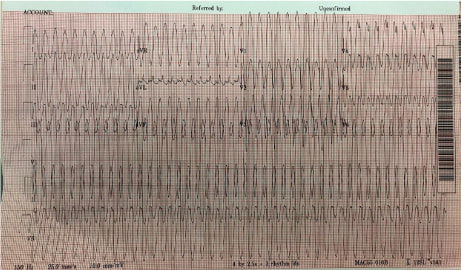
When approaching an EKG with tachycardia, one should first determine: is the QRS complex wide or narrow? And is the rhythm is regular or irregular? This patient’s EKG is regular with a wide QRS complex. Differential Diagnosis - Ventricular Tachycardia, SVT with Aberrancy (Bundle Branch Block or accessory pathway) or paced rhythm. No pacer spikes are seen which leaves VT and SVT with Aberrancy. A number of decision aid tools exist to assist in distinguishing (Brugada is most common) but are cumbersome. What's the final diagnosis?
Wide complex tachycardia likely Idiopathic Monomorphic VT originating from the RVOT. VT = QRS complexes originating in ventricle and > 30 second duration. < 30 second = NSVT. VT is classified as monomorphic (no beat to beat variation in QRS complex morphology) and polymorphic. VT can have ischemic or idiopathic etiologies. This 19 yo was unlikely to have ischemic heart disease. Management?
General Rule - Treat wide complex tachycardias as VT and cardioversion is always the safest option. Per ACLS STABLE patient with wide complex tachycardia that is REGULAR → an adenosine challenge can be attempted. This will terminate SVT and some Idiopathic VTs (eg RVOT). If unsuccessful ⇒ Procainamide Take home points:
1. Differing VT from SVT with aberrancy is not essential. It is always safest to treat as VT.
2. An adenosine challenge may be attempted for WCT only if the following two conditions are met: The patient is STABLE & The rhythm is REGULAR Sources: Link MS, Berkow LC, Kudenchuk PJ et al. Part 7: Adult Advanced Cardiovascular Life Support: 2015 American Heart Association Guidelines Update for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2015; 132:S444
0 Comments
Leave a Reply. |
Categories
Archive
February 2018

Please read our Terms of Use.
|