|
Adapted from Dr. Sarani's Grand Rounds presentation October 5th, 2016  Types of Pelvic TraumaIsolated Pelvis Fractures: relatively good recovery potential Lethal Associated Injuries: Increased risk of blood loss and poor outcomes. Identification of injuries and correct treatment from EMS to the OR is important to treating severe pelvic trauma. Thoracic aorta, intracranial, intra-abdominal Pelvis Fracture Classifications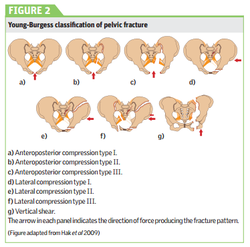 Lateral compression: Most common pelvic fracture. Lateral forces causing fractures of the iliac crest/pubic symphysis Associated with abdominal injuries and low-speed injuries as well as pedestrian struck injuries. AP Compression Fracture: Anterior/posterior pressure with 67% shock and 30% mortality Vertical Shear: vertical traction force due to acceleration/deceleration forces. Causes pubic symphysis disruption and widening. Combined Fracture: Mixture of multiple fracture types.
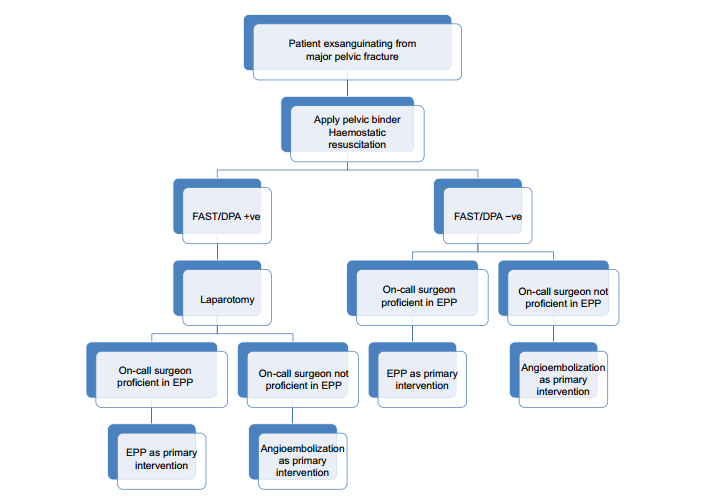 Treatment1. Stop Hemorrhage
2. Disposition
3. Resuscitate in the ICU 4. Morbidity
0 Comments
Leave a Reply. |
Categories
Archive
February 2018

Please read our Terms of Use.
|
||||||