HEART Pathway QI Project
From February 1st-April 1st 2018, a collaborative team of Internal and Emergency residents will be performing an intervention to potentially improve the care of patients presenting for ACS rule-out. During this period, we are asking all Gold Team residents to ask for a HEART score at the time of admission for any ACS rule-out admission. We are also asking for all EM residents to use the HEART Pathway when evaluating patients for ACS rule-out, and use the provided handouts to have a shared decision-making conversation with the patient.
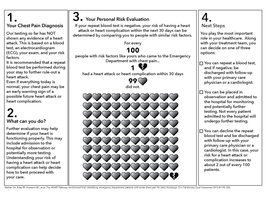
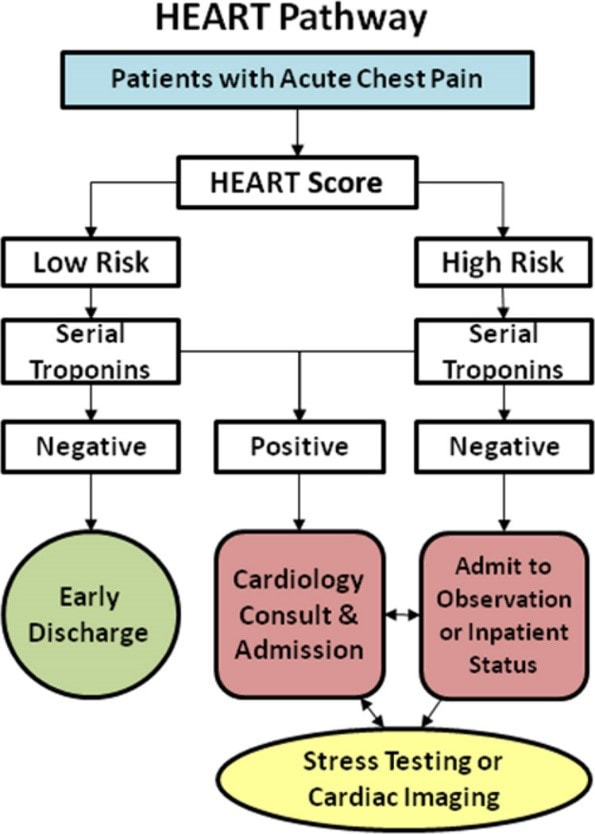
The HEART Pathway is a shared decision making tool that utilizes the HEART score, plus a 3-hour troponin to risk-stratify patients. The HEART Pathway is NOT a sole tool for admission criteria, but a way to help patients understand their risks, and provide patient-centered care. Patients who are given the opportunity to have a shared decision regarding admission for low-risk chest pain more frequently choose discharge over observation, and report increased feeling of safety and engagement with the process.
In a validation study of the HEART Pathway, it was able to reduce cardiac testing, decrease length of stay, and increase early discharges. There was a 99% negative predictive value, with a 1% risk of major adverse cardiac event within 30 days. This is not an insignificant risk, and the patient must understand the risks and benefits of either admission or discharge.
If you have any questions or concerns, please contact Evan Kuhl by TigerText or email.
The HEART Pathway is a shared decision making tool that utilizes the HEART score, plus a 3-hour troponin to risk-stratify patients. The HEART Pathway is NOT a sole tool for admission criteria, but a way to help patients understand their risks, and provide patient-centered care. Patients who are given the opportunity to have a shared decision regarding admission for low-risk chest pain more frequently choose discharge over observation, and report increased feeling of safety and engagement with the process.
In a validation study of the HEART Pathway, it was able to reduce cardiac testing, decrease length of stay, and increase early discharges. There was a 99% negative predictive value, with a 1% risk of major adverse cardiac event within 30 days. This is not an insignificant risk, and the patient must understand the risks and benefits of either admission or discharge.
If you have any questions or concerns, please contact Evan Kuhl by TigerText or email.
|
Documents/Links
Shared Decision Making Macro:
Patient HEART score 0-3, with risk of MACE 2% within 4 weeks, including MI, permanent disability, or death. Other potential causes of the patient's presentation were considered; PERC _. Well's _. Pain not consistent with aortic etiology. Physical exam reassuring without signs of pneumothorax, pulmonary infection, heart failure exacerbation, or respiratory failure. Initial troponin negative. I discussed with patient the results and possibility of approximately 2% of an adverse cardiac event within the next 4 weeks. I offered admission for further monitoring, versus outpatient follow-up with cardiology within the next 5 days. The patient voiced understanding of the risks and benefits of both admission and discharge with rapid follow-up. I discussed return precautions as well, including chest pain, shortness of breath, nausea, near syncope, or other concerning symptoms. After this discussion, the patient elected to _. A prospective validation of the HEART score for chest pain patients at the emergency department. Implementation of a rapid chest pain protocol in the emergency department: A quality improvement project The HEART Pathway randomized trial: identifying emergency department patients with acute chest pain for early discharge. | ||